

BEBCRF Support Group Meeting – Toronto, Fall 2008
An update on the study concerning the long-term efficacy of BOTOX®.
Presenter:
Dr. Harmeet Gill
The guest speaker for the October 19th meeting was Dr. Harmeet Gill who gave an update on the study concerning the long-term efficacy of BOTOX®. The study has been accepted by the American Academy of Ophthalmology for presentation at its annual meeting in November, 2008. It is the world's largest meeting of ophthalmologists, and, the attending specialists come from all parts of the globe. This presentation was partly taken from the University of Toronto's research data and acknowledges the funding and support of BEBCRF.
Dr. Harmeet Gill
Dr. Gill began his presentation by reviewing some basic definitions. Both benign essential blepharospasm (BEB) and hemifacial spasm (HFS) are recognized as facial dyskinesia: the abnormal movement of facial muscles. It is also recognized as a debilitating disorder because it does change people's lives.
BEB is a progressive condition and it generally tends to get worse with time. It is bilateral in that it affects both eyes and is an involuntary contraction of the muscles surrounding the eyes. The contractions cause spasms and the involuntary closing of the eyes. There are other causes that may be attributed to BEB such as dry eyes and they are not to be ruled out of the diagnosis of this condition.
 The Jankovic Scale
The Jankovic Scale
The Jankovic scale is used to measure the progression of this condition. Most physicians will think of blepharospasm in terms of severity and frequency. In some patients the spasms may not be severe but the frequency is quite high due to bright light and, it will impede their ability to read and/or drive. The scale measures up to stage 4 where the severity of the spasms is incapacitating and their frequency renders the person 'functionally blind' more than 50% of the time. Most patients are rated as a stage 2 or possibly 3.
HFS is so named because it involves only one half of the face. It is slightly different in that it involves the 'seventh cranial' nerve located in the brain. This nerve allows the brain to move different parts of your facial muscles. This nerve may be affected by a stroke or a condition called Bell's Palsy, where the face essentially gets droopy. When the nerve gets over-active, it causes spasms: a characteristic of HFS. This nerve controls not only the orbicularis oculi muscles surrounding the outer eye but others going down into the neck.
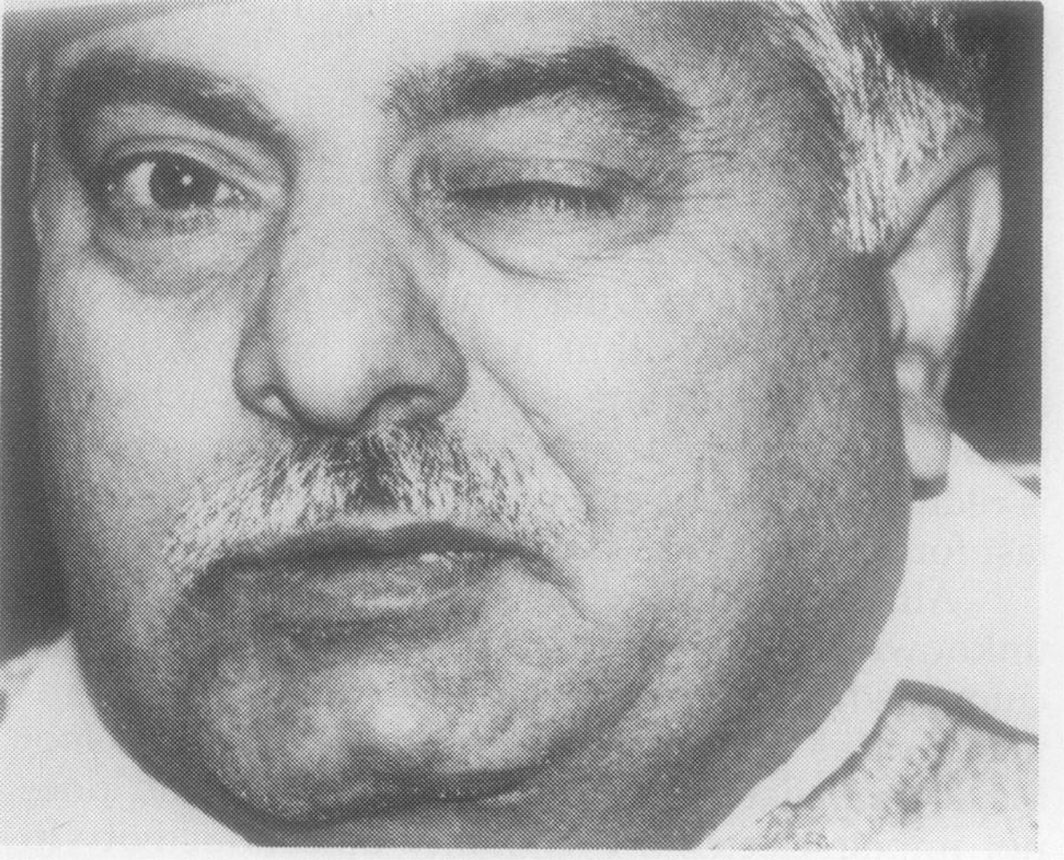 Patient with Left-Sided HFS.
Patient with Left-Sided HFS.
HFS has similar symptoms as BEB. It is often caused by a vascular compression – a blood vessel whose pulsations against the nerve cause it to spasm. Patients suspected of having this condition need to get a CT and MRI examination to verify that this indeed is the case. There are a few cases in the world where people will have bilateral hemifacial spasms and in these rare cases it may be confused with BEB.
In the past, the treatment for BEB often consisted of oral medication and surgery – where the muscles causing the spasms were often 'de-bulked', if you will. However, currently the first-line treatment is botulinum toxin Type A. There are other types of toxin that may be used but the most common is Type A, commonly known as BOTOX®. The general injection time-frame appears to be every three (3) months.
Injections can be done to different parts of the system known as the Orbicularis Oculi muscle. The part which is closest to your eyelid is called the pretarsal (F) followed by the preseptal (E) and the orbital (D). The orbital muscle is the 'forceful' muscle – it is the one that allows you to force-squeeze the eye closed as you would when expelling soap out of your eyes. The pretarsal is specifically involved in the involuntary blink reflex. The eye normally blinks every 12 seconds.
 The muscle anatomy of the Orbicularis Oculi.
The muscle anatomy of the Orbicularis Oculi.
Research has been done, for example the study initiated by Dr. Pang, as to whether injecting the preseptal or the pretarsal muscle would be most beneficial. The effect varies for each individual although it is generally accepted that injecting the pretarsal is a little more effective.
The treatment of injecting botulinum toxin is required for the rest of a patient's life. So, how effective is it going to be over the years? Some believe that the more toxin one gets the less effective it will be over time because one gets anesthetized to the effect. Another theory stipulates that the more toxin the muscles absorb the more atrophied they become; as the treatment progresses less toxin will be required. These are the types of questions that the study hopes to answer.
Dr. Stephen Kraft has meticulously documented the injections his patients received since 1985. Generally a patient receives one injection every 3 months, and, from this medication database the study will extract all those patients that have received 30 consecutive treatments. It is a 'retrospective' or 'longitudinal' study: one that allows us to look back in time and examine the benefits received over a long period of time.
The variable that was examined was the actual number of treatments a patient was receiving and the main beneficial outcome – relief measured in duration of weeks. The study also examined such other things as how did the dosage change, i.e., the actual amount of toxin injected, and, any side effects that might have resulted because of the treatment.
All of the patient records from 1985 to 2007 were examined but the study excluded all those patients who had any hint of secondary causes for their blepharospasm such as apraxia, suffered a movement disorder other than BEB, or, had previous eyelid surgery. This exclusion would allow the study to produce 'clean' statistics that would then become 'generalized'.
The duration of relief was defined as the time from when the patient receives the injection until the time the patient starts feeling the symptoms again. For different people the time span varies anywhere from 5 to 20 weeks. This measurement is variable. Other data that was looked at was the age at which a person started his or her treatment and the type of results obtained; the gender of the patient and the type of the result; the amount of time a person had been receiving the treatment and the type of result; and, the mean dosage amount of the patient.
In total 34 cases were extrapolated from the database: 18 with BEB and 16 with HFS. It was decided not to amalgamate the results because statistically the cases were sufficient in themselves for the purposes of this study. What was examined was the mean duration for the first and last 10 sessions of each case selected.
All of the BEB patients selected had bilateral blepharospasm, and with the HFS patients it was divided evenly – 8 had the left side affected and 8 had the right side affected. Two thirds of the patients were female which is consistent with the literature. Most patients had grade 3 disease as measured by the Jankovic scale.
The mean age for BEB patients in this sample was 51 even though the age range was from 32 to 71 years old. For the HFS patients the range was comparable. The mean age at which patients began getting treatment was 54 for BEB, with a range of 35 to 76, and, 57 for HFS patients. The mean number of treatments for BEB patients was a robust 53 and for HFS it was 48.7. In terms of total years of treatment the mean was 16 years from a range of 10 to 23 years, and, similar results were found with the HFS group.
Overall it was found that there was little significant change between the first and the last 10 sessions, and, perhaps more importantly, the long-term benefits of the treatment remain consistent with little or no side effects.
BOTOX® is a registered trademark of Allergan Corporation